How is renal angioplasty performed?
A local anesthetic is given to the patient at the site of the femoral access and an arterial sheath is inserted into the femoral artery. Under fluoroscopic guidance, a renal guide catheter is positioned in the renal artery through a guidewire. An angiogram is taken and the guidewire is removed.
A contrast dye is injected through a manifold connected to the catheter to obtain an image during cine angiographic recording. Heparin or some other anticoagulant is administered to monitor the clotting time. The guidewire is moved across the renal stenosis. The movement of the guidewire is monitored with the help of fluoroscopy and contrast agent dye.
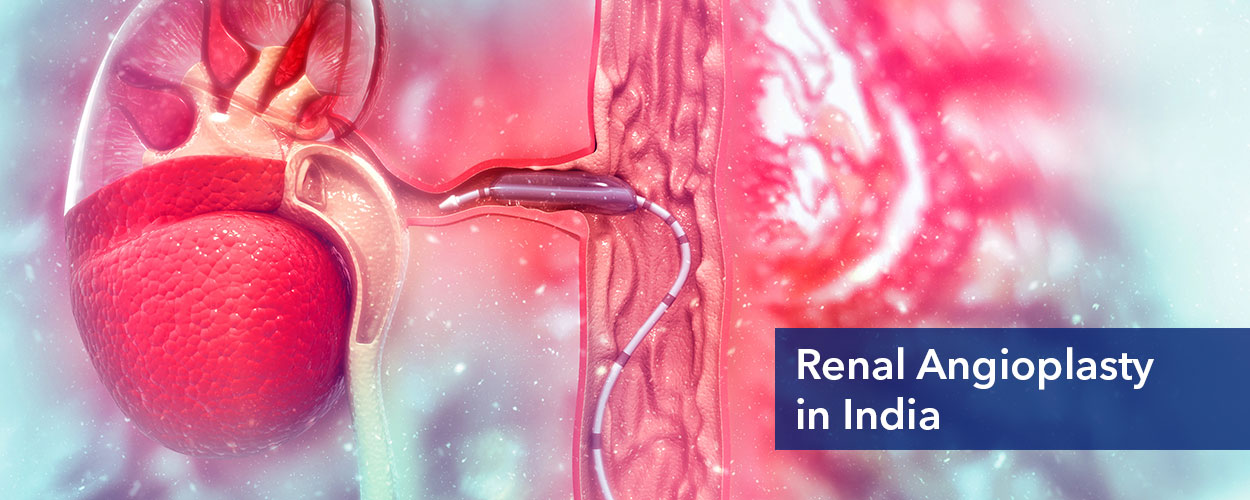
A guidewire is then used to place the balloon across the lesion to keep the artery open. The balloon is already connected to an inflating device containing an equal amount of the contrast agent and saline solution. A negative pressure is applied to the inflating device to expel any air bubbles.
The inflating device is left with the negative pressure and the balloon is moved beyond the distal end of the guide catheter. After placing the balloon, the guide catheter is pulled back gently. A small amount of contrast agent is used to confirm the proper positioning of the balloon.
After confirming the position of the balloon, it is inflated by increasing the pressure using the inflating device. Fluoroscopy is used to see the expansion of the balloon. The expanded balloon is held for a limited amount of time, usually for a few seconds, to apply the pressure on the circumference of the artery.
The balloon is deflated after due course of time and pulled back into the guide catheter. The guidewire is retained and angiography is performed to evaluate the success of the procedure. Blood flow into the renal artery is checked along with any filling defect or dissection in the vascular wall. The guidewire is pulled back after examining the outcome of the procedure.
In the case of a stent-balloon catheter, no negative pressure is applied to the guide catheter. The stent is placed on the lesion and a small amount of contrast dye is used to confirm the position of the stent. A negative pressure is applied to the stent balloon and then it is inflated with the contrast agent-saline solution through the inflation device.
The stent is now left at a particular pressure (5-10 bars) for a few seconds. Then the balloon is deflated and withdrawn by keeping the guidewire retained across the lesion. The stent is left in place to keep the artery open. Specific surgical defects such as filling defects or dissection are checked before withdrawing the guidewire. Angiography is performed to look for any stenosis left in the proximal renal artery. The guide catheter is withdrawn finally from the renal artery.