A craniotomy is typically performed to repair aneurysms and remove brain tumors. A neurosurgeon carries out the surgery.
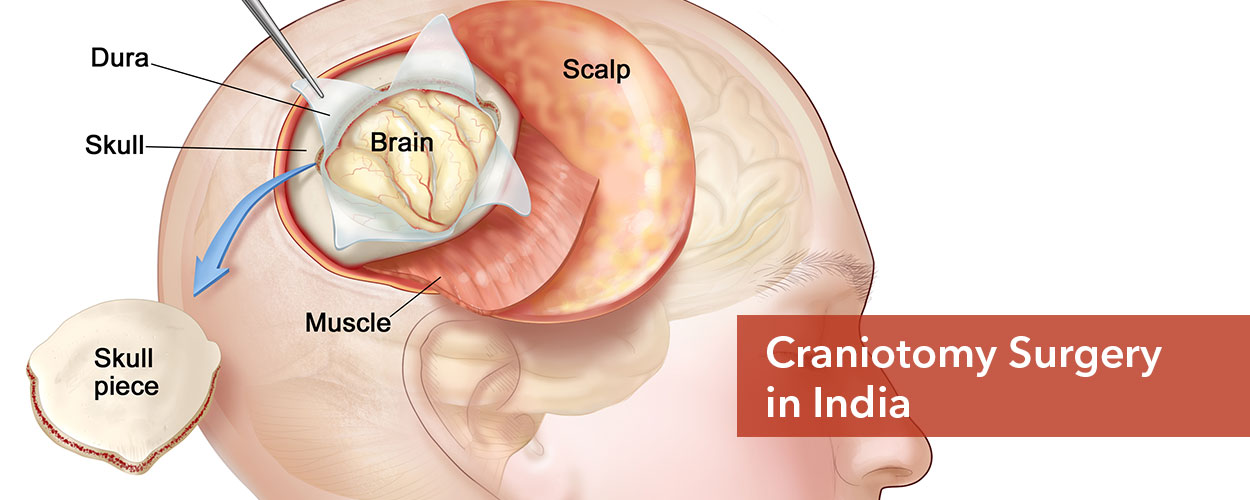
A neurosurgeon makes incisions through the skull and removes a piece of it during a craniotomy to reach the brain. The surgeon reapplies the portion of the skull during the same procedure. This extensive procedure is a craniotomy.
A surgeon usually considers this form of treatment after a brain tumor or other life-threatening disease or after a severe brain injury.
Despite the fact that a craniotomy and a craniectomy are both forms of brain surgery, they are distinct procedures.
- A craniotomy involves removing and replacing a section of the skull in order to gain access to the brain.
- A portion of your skull will also be removed by the surgeon during a craniectomy, but it won’t be placed back in place right away.
- If part of the skull is gone, then one might require a procedure called a cranioplasty as a follow-up procedure.
Craniotomies are named after the part of the skull (cranium) that is removed. The bone flap is replaced or covered with plates and screws after the surgeon has fixed the issue.
So, overall, the treatment is known as a craniectomy if the bone flap is not restored.
In complicated skull base craniotomies, the bone supporting the area of the skull where the cranial nerves, arteries, and veins exit the skull is removed.
Head-and-neck, otologic, or plastic surgeons may be needed in addition to the reconstruction of the skull base.
Image-guidance systems are frequently used by surgeons to plan the access for challenging-to-reach lesions to:
- Remove AVMs or deep brain tumors; clip aneurysms; and any tumors that have invaded the bony skull.
Large decompressive craniectomies are performed to allow the brain to enlarge following a head injury or stroke, despite the fact that most skull holes are kept as small as possible. The bone flap is frozen and restored months later (cranioplasty).